


The interscalene nerve block is a widely used regional anesthesia technique, especially in shoulder and upper arm procedures. One of the most important aspects patients and clinicians want to understand is interscalene nerve block coverage—what areas are affected, how reliable the numbness is, and what limitations exist. Knowing the details of interscalene nerve block coverage helps patients feel confident before surgery and helps clinicians plan anesthesia more effectively.
This article provides a clear, in-depth explanation of interscalene nerve block coverage, how it works, its benefits, limitations, risks, and what patients can expect before and after the procedure.
Introduction to Interscalene Nerve Block Coverage
Interscalene nerve block coverage refers to the specific regions of the body that become numb after the block is administered. This type of block targets the upper portion of the brachial plexus, a network of nerves responsible for sensation and movement in the shoulder and arm.
Unlike general anesthesia, which affects the entire body, interscalene nerve block coverage is localized and controlled. This focused approach makes it particularly useful for surgeries involving the shoulder joint, clavicle, and upper arm. Because of its targeted nature, interscalene nerve block coverage plays a major role in modern pain management strategies.
What Is an Interscalene Nerve Block?
An interscalene nerve block is a regional anesthesia technique in which a local anesthetic is injected near the brachial plexus at the level of the neck. The injection is typically placed between the anterior and middle scalene muscles, where the nerve roots are most accessible.
The goal of the block is to interrupt pain signals traveling from the shoulder and upper arm to the brain. When successful, interscalene nerve block coverage provides both sensory and motor blockade, meaning the area feels numb and may temporarily lose strength.
Today, most interscalene blocks are performed using ultrasound guidance, which improves accuracy and reduces complications. Ultrasound allows the clinician to see nerves, blood vessels, and surrounding structures in real time.
How Interscalene Nerve Block Coverage Works
Interscalene nerve block coverage is achieved by anesthetizing the C5 and C6 nerve roots, and sometimes C7. These nerves supply most of the shoulder joint and the upper portion of the arm.
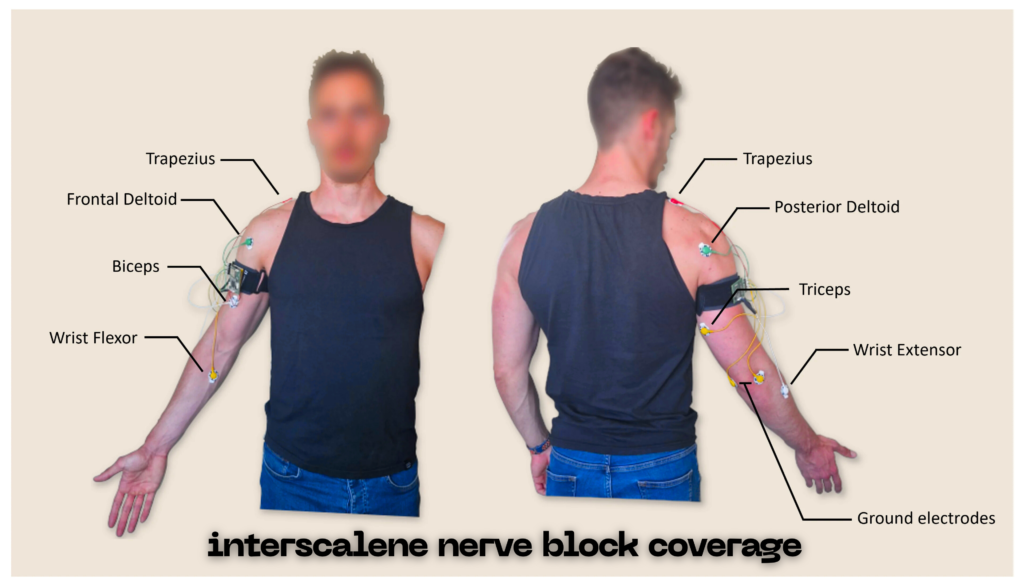
Once the anesthetic spreads around these nerve roots, pain signals are blocked. As a result, interscalene nerve block coverage typically includes the shoulder joint, deltoid muscle, and proximal upper arm. Some patients may also experience numbness near the clavicle or upper chest.
However, it is important to understand that interscalene nerve block coverage is not designed to cover the entire arm. The lower nerves of the brachial plexus, which control the forearm and hand, are often not affected.
Interscalene Nerve Block Coverage – Quick Bio Table
| Field | Details |
|---|---|
| Medical Name | Interscalene Nerve Block |
| Type | Regional anesthesia technique |
| Primary Coverage Area | Shoulder, upper arm, clavicle |
| Nerve Roots Involved | C5–C6 (sometimes C7) |
| Common Use | Shoulder and upper arm surgery |
| Pain Relief Duration | 6–12 hours (longer with catheter) |
| Procedure Method | Ultrasound-guided injection |
| Main Benefit | Strong pain control, reduced opioids |
| Limitations | Limited hand and forearm coverage |
| Performed By | Anesthesiologist |
| Risk Level | Low when ultrasound-guided |
Areas Affected by Interscalene Nerve Block Coverage
The primary areas included in interscalene nerve block coverage are the shoulder and upper arm. This makes the block ideal for procedures that focus on these regions.
Patients can expect numbness in the shoulder joint itself, including deep structures inside the joint. The deltoid region and the upper part of the humerus are also commonly affected. Depending on anesthetic spread, interscalene nerve block coverage may extend to the collarbone area.
In contrast, the elbow, forearm, wrist, and hand are usually not fully covered. This selective coverage is intentional and helps avoid unnecessary numbness in areas not involved in surgery.
Common Uses of Interscalene Nerve Block Coverage
Interscalene nerve block coverage is most commonly used in shoulder surgeries. These include rotator cuff repair, shoulder arthroscopy, labral repair, and total shoulder replacement.
The block is also used for surgeries involving the proximal humerus or clavicle. In addition to surgical anesthesia, interscalene nerve block coverage is widely used for post-operative pain control, often lasting several hours after surgery.
In some cases, the block may be used for acute pain management, such as severe shoulder injuries or dislocations, particularly when reducing the need for heavy sedation is desirable.
Benefits of Interscalene Nerve Block Coverage
One of the biggest advantages of interscalene nerve block coverage is excellent pain control. By targeting pain at its source, patients often experience significantly less discomfort after surgery.
Another major benefit is the reduction in opioid use. Because pain is managed locally, patients may require fewer opioid medications, lowering the risk of nausea, dizziness, constipation, and dependence.
Interscalene nerve block coverage also supports faster recovery. With better pain control, patients are often able to begin gentle movement and physical therapy sooner, which improves long-term shoulder function.
Duration of Interscalene Nerve Block Coverage
The duration of interscalene nerve block coverage depends on the type and dose of anesthetic used. In most cases, numbness lasts 6 to 12 hours.
Some patients may receive additives or a continuous nerve catheter, which can extend interscalene nerve block coverage for 24 hours or longer. Extended coverage is particularly helpful after major shoulder surgeries, where pain can be intense in the first post-operative day.
As the block wears off, sensation and strength gradually return. This process is normal and expected.
Limitations of Interscalene Nerve Block Coverage
While interscalene nerve block coverage is highly effective for the shoulder, it has clear limitations. It does not reliably numb the forearm or hand, making it unsuitable as a sole anesthetic for surgeries below the elbow.
Patients undergoing procedures involving the hand or wrist may need additional nerve blocks to supplement interscalene nerve block coverage. This limitation should be discussed during pre-operative planning.
Another limitation is temporary muscle weakness in the shoulder and arm, which can affect mobility for several hours.
Risks and Side Effects
Although generally safe, interscalene nerve block coverage is associated with some potential side effects. Temporary diaphragm weakness can occur due to involvement of the phrenic nerve, which may cause mild shortness of breath in some patients.
Other possible effects include drooping of the eyelid, facial warmth, or hoarseness, which are usually temporary. Rare complications include nerve injury, bleeding, infection, or lung puncture.
Using ultrasound guidance and proper technique significantly reduces these risks and improves the safety of interscalene nerve block coverage.
Who Is a Good Candidate for Interscalene Nerve Block Coverage
Most adults undergoing shoulder or upper arm surgery are good candidates for interscalene nerve block coverage. Age alone is not a limiting factor, as the block can be safely used in both younger and older patients.
Patients with severe lung disease, previous neck surgery, or certain anatomical variations should discuss risks and alternatives with their anesthesiologist. A thorough evaluation ensures that interscalene nerve block coverage is both safe and effective.
What to Expect After the Block
After receiving the block, patients typically feel numbness and heaviness in the shoulder and upper arm. Pain is often minimal or completely absent during the initial hours.
Patients should protect the numb limb from injury and avoid lifting or driving until sensation returns. As interscalene nerve block coverage wears off, pain medication may be needed to maintain comfort.
Proper post-operative instructions help ensure a smooth recovery and prevent complications.
Conclusion
Interscalene nerve block coverage is a powerful and effective tool in modern anesthesia. By providing targeted numbness to the shoulder and upper arm, it offers excellent pain control, reduces opioid use, and supports faster recovery.
While interscalene nerve block coverage has limitations, particularly below the elbow, it remains the gold standard for shoulder surgery anesthesia and pain management. Understanding how it works, what it covers, and what to expect allows patients to approach surgery with confidence and clarity.
For anyone preparing for shoulder surgery or managing severe shoulder pain, discussing interscalene nerve block coverage with an experienced anesthesiologist can make a significant difference in comfort, safety, and overall recovery.
FAQs
Q: What areas does the interscalene nerve block numb?
A: It primarily numbs the shoulder, upper arm, and part of the clavicle, but usually does not affect the forearm or hand.
Q: How long does the pain relief last?
A: Typically, 6–12 hours, depending on the anesthetic used; a continuous catheter can extend relief up to 24 hours or more.
Q: Is the procedure safe for all adults?
A: It is generally safe for most adults, but patients with lung problems or prior neck surgery should consult an anesthesiologist first.
Q: Will I be fully asleep during the block?
A: No, the block provides regional numbness; patients can remain awake or lightly sedated during the procedure.
Q: What are common side effects?
A: Temporary weakness in the shoulder or diaphragm, drooping eyelid (Horner syndrome), or mild numbness; serious complications are rare with ultrasound guidance.
